The following list of "frequently asked questions" help guide you in using the basic and advanced functions of the ezScriptWriter software:
Before using ezScriptWriter the first time a password needs to be established. On the main login screen, choose “Password Options” and enter your username in both the username and password fields (the assigned username is the user's first initial plus last name). Enter a new password and re-enter to confirm (losing or forgetting a password would require it to be reset by the administrator). If you leave the password field blank, you will default to no password (not recommended!). You will be returned to the login screen and you must re-enter the new password.
Specific HIPAA compliance features built into ezScriptWriter:
· Time-based automatic logout with keyboard inactivity
· Physician review/authorization of staff-entered patient data
· Extensive logging of patient data changes
· Patient-requested removal of personal data
· Transaction logging/audit trail for all users
· Comprehensive printable patient file
Occasionally, a patient may neglect to pay the balance due the office. While the billing process is proceeding, a method to mark the prescriptions so that they are not dispensed until the balance is paid is included in ezScriptWriter. Just right-click on the Rx in the encounter view (as shown below) and choose “Hold” from the pop-up menu. Follow the prompts and the Rx will be marked as status “HOLD” until released; this prevents inadvertent release of the Rx by a staff member unaware of the billing status of the patient.
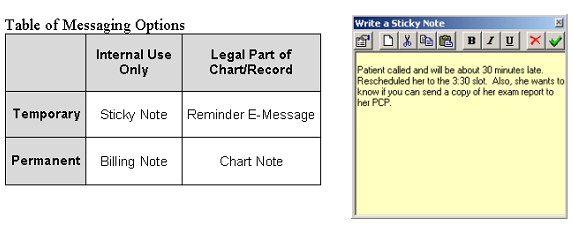
ANSWER: Besides the standard "SOAP encounter", ezScriptWriter allows several different methods to document non-exam events such as telephone calls, billing issues, and reminders. The grid below explains the possibilities:
Sticky Note: Resembling the ubiquitous sticky notes that clutter most desks, this is an electronic version for brief, non-clinical messages. Examples might include: a note to the doctor that the patient is running late, that a patient seems annoyed about waiting so long, or a reminder that results need reviewed before finalizing the record. Both the front desk staff and the clinical staff can make use of sticky notes. The sticky note is temporary (deleted automatically when the chart is re-filed) and is for internal use only (not appropriate for clinical information).
Billing Note: For use mostly by front desk staff, the billing note allows for brief documentation of billing issues, disputes, insurance discrepancies and collection problems. Short transcripts of telephone conversations about billing issues would be appropriate as well. The billing note is part of the permanent chart (saved each time it is modified) and is for internal use only (not printed as part of the patients chart record).
Reminder E-Message: A reminder E-message is very similar in format to an email message. Generated either by the clinical staff or the front desk staff, the message is timed to appear at some specified future date. Examples would include reminders to have a patient come in for visual field testing, to notify the doctor to review a consultation report due back, or a reminder to schedule an uncompleted contact lens follow-up appointment. The reminder message is temporary (in the sense that it is visible only during a discreet time period), but it is part of the legal chart (once the final disposition is indicated, the reminder message text is appended to the general chart notes).
Chart Note: The chart note is for additional clinical information. For example, telephone conversations regarding clinical data (e.g. medication refills, contact lens complaints, etc) would be described in the time-stamped chart note. Other uses include brief discussions of lab results, consultation visits, record review, and notation of missed patient appointments (and the actions taken). The chart note is legal record that becomes part of the permanent chart (requires signing by an authorized signer).
Any of the note methods are available from the Pulled Charts list. Right-click on the patient name and select “Message Manager” to bring up the appropriate choices.